60Y /F WITH RIGHT UPPER AND LOWER LIMB WEAKNESS WITH DEVIATION OF MOUTH TO LEFT
This is an online e-log book to discuss our patient's de-identified health data shared after taking his / her / guardian's signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
This E blog also reflects my patient-centered online learning portfolio and your valuable input in the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and coming up with diagnosis and treatment plans. is an online e-log book to discuss our patient's de-identified health data shared after taking his / her / guardians' signed informed consent. Here we discuss our individual patients' problems through a series of inputs from the available global online community of experts with an aim to solve those patients' clinical problems with collective current best evidence-based information.
20/9/23
This is a case of 60y old female brought to casualty with c/o loss of consciousness since 1 hour,right lower and upper limb weakness since today afternoon ,deviation of mouth towards left side .
Hopi:
Patient was apparently asymptomatic till today when patient attender came to home patient is in unconscious state ,with right lower and upper limb weakness, with deviation of mouth towards left .
No h/o head ache ,fever ,vomitings
N/k/c/o DM,HTN,CAD,TB ,EPILEPSY
Past history:
patient had similar episode 5 years back and was treated here advised for referring to higher centre but due to financial status they went to local hospital and given medication and she recovered then
K/C/O hypertension since 30 years
N/k/c/o DM,CAD,TB ,EPILEPSY
PERSONAL HISTORY:-
Diet - mixed
Appetite- normal
Sleep - adequate
Bowel and bladder -regular
Addictions- not present
Allergic history:- No history of any kind of allergies for food/drugs
Family history:- no significant family history
GENERAL EXAMINATION:-
Patient is drowsy ,in coherent
NO PALLOR ,ICTERUS; CLUBBING; CYANOSIS; ; LYMPHADENOPATHY ; EDEMA

Systemic examination:
Cvs-s1,s2 heard
Rs -Bae present
P/a -soft,nt
CNS examination:
Patient is drowsy ,incoherent,but arousable
Bp-160/90 mmHg
Pr-88 bpm
Rr-22 cpm
GCS -E3V2M5
Pupils-both mildly reacting to light
Power: right. left
U/l. 0/5. 3/5
L/l. 0/5. 3/5
Tone.: right. . Left
U/l. Increased normal
L/l. Increased. Normal
Reflexes: right left
B. +++. +++
T. ++. ++
S. +. +
K. +++. +++
A. ++. ++
P increased. Increased
Hemiplegic gait
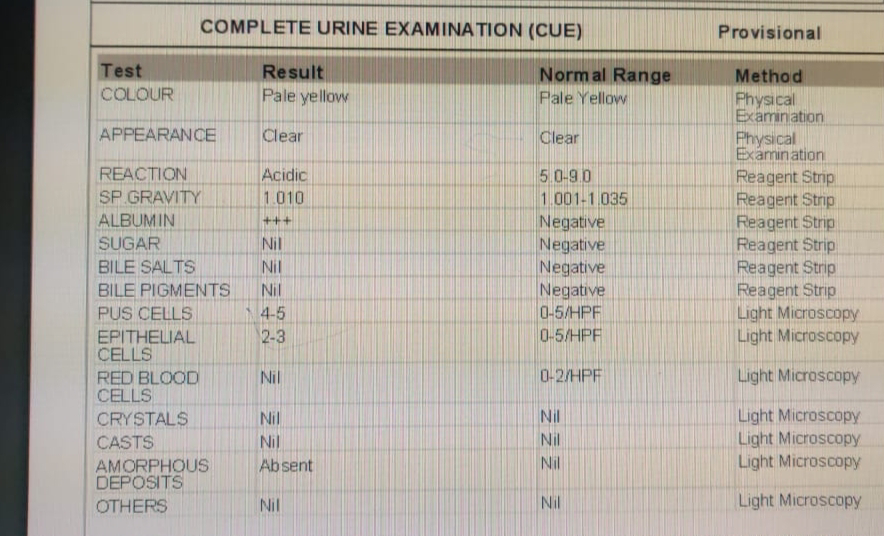
INVESTIGATIONS:





MRI brain:



Diagnosis:
ACUTE HEMORRHAGIC STROKE ?
WITH K/C/O HTN SINCE 30 YEARS

Comments
Post a Comment